

Physical activity generally decreases as people age, which allows hypokinetic diseases to ravage older populations.
I’m older than 86 percent of the Earth’s population. I’m an aging academic. I’m an aging parent. I’m an aging worker. I’m an aging trainee. And I am part of one of the largest segments of our population: 33 percent of us are over 50 years of age. If you look at any textbook within exercise academia, you will generally find aged individuals, older individuals and geriatric populations—basically people like me—listed as a “special population.”
I do not require kid-glove treatment because of my age. I will not break in response to progressive training because of my age. I am not magically disabled simply because of my age. I am not special.
So what do people really mean when they refer to older individuals as a “special population”?
CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS
An Incorrect Association
The term “special population” is a catch-all used by academic exercise organizations to describe diseased populations that require modifications to their training, and, strangely, healthy populations that might or might not require modifications to their training other than simple scaling.
According to the National Strength and Conditioning Association those groups most commonly assigned the special-population moniker are those that have:
- Cardiovascular disease
- Pulmonary disease
- Metabolic disease
- Immunological disease
- Musculoskeletal disease
- Neuromuscular disease
- Cancer
- Psychological/behavioral disorder
The list also includes three other groups:
- Those who are pregnant
- Children and adolescents
- Older adults
Neither pregnancy nor adolescence is a disease, and these categorizations are clearly not appropriate. Pregnancy is a healthy biological function, although it does require some modifications in exercise practice. And although W.C Fields might have considered children a disease, kids are anabolic little beasts who require progression and exposure to broad exercise demands. Being a kid is not a disease.

CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS!
Most government activity recommendations are bare minimums. By training to improve fitness, older adults give themselves the best chance to maintain health and independence in their later years.
We can also exclude the first eight items on the list above. After all, the term “diseased population” is already correctly applied, so we need not call them “special” and apply two names to the same thing.
Where aging is concerned, we know chronology is correlated to mortality: The more days you live, the closer your date of death. But that doesn’t make aging a disease. The one thing that likely puts older adults into the category of diseased populations is a choice: We drop out of physical activity for the comfort of the couch.
The one thing that likely puts older adults into the category of diseased populations is a choice: We drop out of physical activity for the comfort of the couch.
This choice is still not a disease, but consider that by the time the 50th birthday rolls around, only about one in six of us is still exercising and active to the minimal levels suggested to maintain health. The data only worsens as we reach our 60th and 70th birthdays.
{target=_blank} )](https://d1s2fu91rxnpt4.cloudfront.net/mainsite/m20161018185907/display/CHANGE%2520IN%2520PARTICIPATIOVER%2520LIFESPAN-2.jpg)
CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS!
Figure 1: Self-reports of physical activity generally show that activity levels drop over the lifespan. Note the significant drop-off after 50 for those classified as physically active (those who exercise, play sports or do other physical activity at a very low frequency). People who already train or play sport regularly tend to continue doing so until age 60, when participation drops significantly. [(Source: Scottish Government)] (http://www.gov.scot/Publications/2006/09/29134901/4)
That choice to become less and less fit over time sets up the opportunity for hypokinetic diseases to gain a foothold and become statistically correlated with old age. Hypokinetic diseases are those that are associated with the lack of habitual physical activity or exercise in one’s lifestyle.
If you choose to become inactive with age, you choose to make yourself more vulnerable to disease and to be lumped into the “special” diseased group. But in reality it is the presence of disease that makes such individuals special, not age.
If you actually think about it, older couch potatoes are not special in any sense of the word. Instead, they are becoming a part of the diseased majority, the nearly two-thirds of the population who do not exercise.
If you choose to become inactive with age, you choose to make yourself more vulnerable to disease.
The presence of hypokinetic diseases in older populations is profound. When we look at the diseases on the previous list, the frequency of occurrence in most instances appears to be linked to aging but is more strongly linked to inactivity.
When we look at the incidence of cardiovascular disease by age group, younger adult to older adult, we see a step-wise increase in the diagnosis of the disease (1). We see a very similar situation with the frequency of diagnosed pulmonary disease over the later lifespan. Further, we see an increase in the occurrence of overlapping pulmonary diseases. At age 40, about 20 percent of those with asthma will also have obstructive pulmonary disease. By age 70 that number rises to about 67 percent (2). We see similar frequency increases in metabolic disease (3), immunological disease (4), musculoskeletal disease (5), neuromuscular disease (6,7), cancer (8) and psychological disorders (9).
And this is not new knowledge. As early as 1922, the relationship between physical inactivity and certain types of diseases— those special-population diseases listed above—had been noted (10,11). The term “hypokinetic diseases,” coined in 1954, was the subject of a 1961 textbook that described diseases and conditions that had a statistical association with lack of exercise or lack of other physical activity (12). The original 1954 list of hypokinetic diseases included heart disease, obesity, diabetes, arthritis, joint problems, depression, mental disorders, back pain and some cancers.
It’s easy to see how confusion creates the idea that aging is a disease process: The elderly seem to be riddled with diseases. The almost geometric increase in the frequency of hypokinetic diseases after 40 paints a rather stark portrait of my later years if I am within the norm. But I’m not, and no one has to be.
CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS!
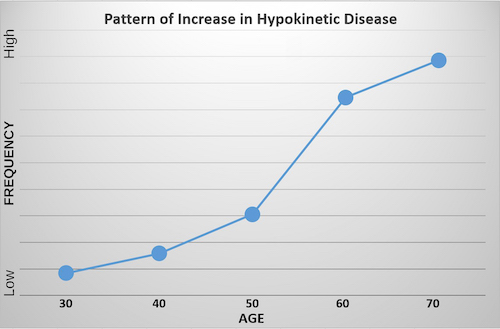
Figure 2: The general pattern of increase in the occurrence rate of hypokinetic diseases. The absolute numbers of those affected by the individual diseases vary, but when the diseases are looked at as a group, a shared pattern of increase in disease occurrence in the last half of the lifespan can be seen. (Graphic represents pooled frequency patterns in references 1-9.)
Getting Old, Getting Sick
When we look at how many people are completely sedentary— physically inactive—we see a nearly geometric increase in the number of people over 40 who are absolutely physically inactive. This increase very nearly mirrors the increase in the frequency of hypokinetic diseases. And this is the important part: As physical activity decreases, the frequency of hypokinetic diseases increases (compare Figure 1 and Figure 2).
So we have a question: Is age directly linked to increased frequencies of disease or does simply being a couch potato create a more easily deranged set of cellular, tissue, system and organismic circumstances that allow disease processes to become established?
The tendency in current literature seems to indicate that those with more robust physical-activity and exercise histories—interpreted as higher fitness—have fewer hypokinetic diseases and a lower death rate than those who are physically inactive (13). But we have little data on the occurrence of disease over lifespan when exercise is held constant at levels that induce fitness gain or maintain high levels of fitness. The data we have on exercise frequency and intensity is generally derived from self-report, a low-reliability method of determining biological relationships. This means a lot of guesswork is employed when it comes to the absolute effects of exercise on aging.
Over the past century, many government initiatives have attempted to improve the fitness of the U.S. population and populations in other countries, but they have all been abysmal failures if you review current statistics on the outcomes for exercise, physical activity, obesity and hypokinetic diseases. Things have gotten worse, not better. This is generally because all the efforts focus on the lowest amount of physical activity needed to avoid disease rather than addressing the need for fitness to accomplish the desired improvements in function and health.
You—the master of your own destiny—need to do what the government couldn’t: Take control of your and your trainees’ fitness in order to improve life functions and quality of life and stave off the development of hypokinetic diseases.
We aren’t destined for hypokinetic diseases just because we get old.
Given that fitness seems to prevent and in many instances cause a regression in disease processes, it would be very tempting to say that exercise acts as a proxy for medical interventions and then say “exercise is medicine.” Lots of other people and organizations do this, but they are simply fooling themselves and the public.
Creating fitness is not the same as prescribing a dose of penicillin. Creating fitness is its own end. It is, as CrossFit Founder and CEO Greg Glassman terms it, “non-medical health care.”
We don’t need a medical or clinical degree to deliver fitness and its preventive benefits. We only need to be able to create fitness and deliver it effectively and reliably to those who need it most. That is actually everyone who does not exercise currently. But considering the previous discussion, and with reference to Figure 1, we should strongly consider ways to keep people 50 and older coming to the gym, training at home or in some way exercising regularly.
A Head-Start Program for Adults
Some bright spots exist. Although some drop out of regular training as they age, physical function and the occurrence of hypokinetic diseases in later life is affected by the actions of our younger selves. Being fit at younger ages provides an advantage in later life by establishing a base resistance to disease processes. If we are fit in adulthood, experimental data suggests we are less likely to become diabetic as we age (14). This effect can become even more powerful if combined with appropriate nutritional habits.

CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS!
While far too many spend retirement in the rocking chair, the wise use their free time to ensure the golden years are full of vitality.
Other research is suggestive that fitness gained in adulthood can delay the onset of age-related increases in blood pressure by about a decade (15). Hypertension is one of the important risk factors associated with developing cardiovascular disease, and it affects a large segment of society. Delaying or eliminating the onset of hypertension is valuable, and spending time in the gym training during younger adulthood seems to be an easy way to do this.
It’s never too late for anyone, regardless of exercise history, to start a journey toward fitness.
If being previously fit delays the onset of later-life hypokinetic disease, gym time in the younger years is a boon for everyone. If pre-conditioning extends the lifespan by a decade, then we can potentially cut the number of 50- and 60-year-olds who are experiencing the onset of hypokinetic diseases significantly, an effect that might decrease the severity of disease in the over-70s.

CLICK HERE TO LEARN ABOUT OUR LEGENDS CLASS!
Figure 3: The blue line represents the increase in hypokinetic disease rate seen if the individual is historically sedentary. The green line represents the increase in hypokinetic disease rate in individuals who have a previous training history in adulthood but do not currently train. Note that a residual effect of previous fitness might delay disease onset by up to a decade. (Graphic represents pooled frequency patterns in references 1-9,14,15.)
We can’t truly think that all the fitness gained early in life will persist across decades. It doesn’t. We have all experienced de-training first hand. When we get fit and then stop training, we get unfit. We might experience some residual biological effects, but the majority of things that make us better and more functional can be lost in days, weeks, months and years (16,17,18,19). The obvious point is that if you want to ensure you have the best chance to avoid hypokinetic diseases and maintain quality of life, you should not get fit then stop training. We actually need to continue training when we are older.
A less obvious point is that it’s never too late for anyone, regardless of exercise history, to start a journey toward fitness.
Playing Catch-Up
It is never too late to get up off the couch and start training to improve strength, endurance and mobility. Although each of these elements of fitness is exquisitely developed by CrossFit training, any system of exercise can be used as long as it is progressive and improves fitness in some aspect.
Being stronger is associated with longevity (20). Higher endurance is associated with longevity (21). Mobility is associated with longevity (22). Although the available research cannot prove causality here, the weight of the correlations provides us with a good sense of direction in how we should approach exercise and aging.
Get your aging self to the gym with grandpa and grandma and mom and dad—that’s the approach.
When an older adult starts training, the results can be spectacular. Strength levels can increase by 23 percent in as little as 12 weeks even in those up to 92 years of age (23). Endurance levels can increase by 16 percent in as little as four months (24). Mobility can improve, too, with a significant 62 percent reduction in falls seen after a year of training (25). And when we bundle those outcomes together, we find that not only are physical function and quality of life improved, but creating fitness in older adults also cuts the risk of disease and death significantly.
Simply put, the concept that older trainees cannot adapt to training has no merit. Similarly flawed are recommendations that older trainees aspire to only the lowest levels of physical activity— the bare minimums. If higher fitness is related to lower disease and death rates, then we should use methods that create those levels of fitness.
A Different Kind of Special
If you don’t want to be part of a “special population,” don’t sit on your butt. Get to the gym.
I refuse to be that kind of special. And I want the exercise industry to stop using that term to describe older adults just because of an erroneously assumed relationship between aging and disease. We need to stop the automatic treatment of the aging as feeble and infirm, and we need to end to the widespread creation of physical-activity programs that do nothing to delay or stop fitness decay.
I do, however, want to be a different kind of special. I want to be the kind of special that’s earned in the gym, the kind of special that allows you to be capable of the things often considered the province of the young. Maintaining a high level of function sets you apart from the average non-exercising older adult, and it will help keep you disease-free and allow you to enjoy a long life.
References
- ISD Scotland. Health Conditions: General Practice. Available athttp://www.isdscotland.org/Health-Topics/General-Practice/ GP-consultations/Health-Conditions/CHD/. Accessed Sept. 21, 2016.
- Rhee CK. Phenotype of asthma-chronic obstructive pulmonary disease overlap syndrome. The Korean Journal of Internal Medicine, 30(4): 443-449, 2015.
- Toto RD, Sowers JR, Jamerson KS. A debate on the metabolic syndrome: Evolving challenges and controversies. Medscape Multispeciality CME. CE 511929, 2005.
- Broadley SA, Deans J, Sawcer SJ, Clayton D, Compston DAS. Autoimmune disease in first-degree relatives of patients with multiple sclerosis. A UK survey. Brain, 123: 1102-1111, 2000.
- The United States Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States: Prevalence, Societal and Economic Cost (3rd Edition). Rosemont, Ill.: 2014.
- Dewey RB. Overview of Parkinson’s Disease. Available at http://parkinsonsed.com/pd-dialogues/parkinsons-disease-overview Accessed Sept. 21, 2016.
- Us Against Alzheimer’s. The Crisis. Available at http://www. usagainstalzheimers.org/crisis. Accessed Sept. 21, 2016.
- Buck Institute. Aging and Cancer: An Unexpected Pair. Available at http://sage.buckinstitute.org/aging-and-cancer/. Accessed Sept. 21, 2016.
- National Institute of Mental Health. Serious mental illness (SMI) among U.S. adults. Available at: http://www.nimh.nih. gov/health/statistics/prevalence/serious-mental-illness-smiamong-us-adults.html. Accessed Sept. 21, 2016.
- Allison N and Brooks B. Bone atrophy: A clinical study of the changes in bone which result from nonuse. Archives of Surgery 5: 499, 1922.
- Dock W. The evil sequelae of complete bed rest. Journal of the American Medical Association 125(16): 1083-1085, 1944.
- Kraus H and Raab W. Hypokinetic Disease: Diseases Produced by Lack of Exercise. Springfield, Ill.: Thomas, 1961.
- Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, Milani RV, Blair SN, Church TS. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circulation Journal 77(2): 281- 292, 2013.
- Chow LS, Odegaard AO, Bosch TA, Bantle AE, Wang Q, Hughes J, Carnethon M, Ingram KH, Durant N, Lewis CE, Ryder J, Shay CM, Kelly AS, Schreiner PJ. Twenty year fitness trends in young adults and incidence of prediabetes and diabetes: The CARDIA study. Diabetologia 59(8): 1659-1665, 2016.
- Liu J, Sui X, Lavie CJ, Zhou H, Park YM, Cai B, Liu J, Blair SN. Effects of cardiorespiratory fitness on blood pressure trajectory with aging in a cohort of healthy men. Journal of the American College of Cardiology 64(12): 1245-1253, 2014.
- Liao YH, Sung YC, Chou CC, Chen CY. Eight-week training cessation suppresses physiological stress but rapidly impairs health metabolic profiles and aerobic capacity in elite taekwondo athletes. PLoS One 11(7): e160167, 2016.
- Waring CD, Henning BJ, Smith AJ, Nadal-Ginard B, Torella D, Ellison GM. Cardiac adaptations from 4 weeks of intensity-controlled vigorous exercise are lost after a similar period of detraining. Physiological Reports 3(2). pii: e12302, 2015.
- Zech A, Drey M, Freiberger E, Hentschke C, Bauer JM, Sieber CC, Pfeifer K. Residual effects of muscle strength and muscle power training and detraining on physical function in community-dwelling prefrail older adults: A randomized controlled trial. BMC Geriatriatrics 12: 68, 2012.
- Heinonen A, Mäntynen J, Kannus P, Uusi-Rasi K, Nikander R, Kontulainen S, Sievänen H. Effects of high-impact training and detraining on femoral neck structure in premenopausal women: A hip structural analysis of an 18-month randomized controlled exercise intervention with 3.5-year follow-up. Physiotherapy Canada 64(1): 98-105, 2012.
- Ruiz JR, Sui X, Lobelo F, Morrow JR Jr, Jackson AW, Sjöström M, Blair SN. Association between muscular strength and mortality in men: Prospective cohort study. British Medical Journal 337: a439, 2008.
- Lee DC, Sui X, Artero EG, Lee IM, Church TS, McAuley PA, Stanford FC, Kohl HW, Blair SN. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: The Aerobics Center Longitudinal Study. Circulation 124(23): 2483-90, 2011.
- Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clinics in Geriatric Medicine 18: 141–158, 2002.
- Yarasheski KE, Pak-Loduca J, Hasten DL, Obert KA, Brown MB, Sinacore DR. Resistance exercise training increases mixed muscle protein synthesis rate in frail women and men >/=76 yr old. American Journal of Physiology 277 (1 Pt 1): E118-125, 1999.
- Tsuji I, Tamagawa A, Nagatomi R, Irie N, Ohkubo T, Saito M, Fujita K, Ogawa K, Sauvaget C, Anzai Y, Hozawa A, Watanabe Y, Sato A, Ohmori H, Hisamichi S. Randomized controlled trial of exercise training for older people (Sendai Silver Center Trial; SSCT): Study design and primary outcome. Journal of Epidemiology 10(1): 55-64, 2000.
- Karinkanta S, Kannus P, Uusi-Rasi K, Heinonen A, Sievänen H. Combined resistance and balance-jumping exercise reduces older women’s injurious falls and fractures: 5-year follow-up study. Age and Ageing 44(5): 784-789, 2015.
About the Author: Lon Kilgore earned a Ph.D. from the Department of Anatomy and Physiology at Kansas State University’s College of Veterinary Medicine. He has competed in weightlifting to the national level since 1972 and coached his first athletes from a garage gym to national-championship event medals in 1974. He has also competed in powerlifting, the first CrossFit Total event, wrestling and rowing. He has worked in the trenches, as a qualified national-level coach or scientific consultant, with athletes from rank novices to the Olympic elite, as a small business owner, and as a consultant to fitness businesses. He was co-developer of the Basic Barbell Training and Exercise Science specialty seminars for CrossFit (mid-2000s) and was an all-level certifying instructor for USA Weightlifting for more than a decade. He is a decorated military veteran (sergeant, U.S. Army). His illustration, authorship and co-authorship efforts include several best-selling books and works in numerous research journals. After a 20-year professorial career in higher academia, he currently delivers vocational-education courses (some for free) through the Kilgore Academy, provides online commentary and analysis of exercise-science papers, and works as a writer and illustrator.